Professor Dr. med. Christian ScharfetterDept. of Psychiatry, Psychotherapy & PsychosomaticsPsychiatric Hospital, University of Zurich |
|
|
NosologyThe strength of modern diagnostic systems in psychiatry lies in nosology, that is, in the systematic collection of knowledge and in the description and differentiation of the complex phenomena which become manifest as psychiatric disorders. In consequence, the well-established diagnostic systems ICD-10 and DSM-IV have achieved a high degree of perfectionism, thus representing state-of-the-art instruments for the daily work of clinicians worldwide. Yet these diagnostic systems do not offer clinicians reliable guidelines for therapy and prognosis for a particular patient. In consequence, it is currently impossible to make any prediction of how a particular patient will respond to a particular antipsychotic or antidepressant therapy. EtiologyLittle is known about the etiology of functional psychoses. Even though strong evidence from adoption and twin studies underlines the significance of genetic contributions to the development of these illnesses, the usefulness of psychiatric diagnoses for genetic studies is rather limited, as they delineate the familial aggregation of syndrome patterns insufficiently and do not elucidate the modes of genetic transmission from one generation to the next. Quantitative ApproachesMultidimensional quantitative approaches to disentangling the complex processes that underlie psychiatric disorders, their development, acute phase, and further course, apparently offer advantages over the qualitative taxonomy of diagnostic systems. Empirical data from our studies carried out over the past two decades clearly support this view, as quantitative syndrome patterns have turned out (1) to resolve the fine gradations of within-family psychopathologies that do nor reach diagnostic thresholds, (2) to model genetic predisposition across ethnicities well compared with epidemiologic data, (4) to relate to the time course of recovery under psychotropic drug treatment, and (5) to lead to a generalized model of genetic vulnerability to functional psychoses, where none of the vulnerability factors by itself is necessary or sufficient for the development of the disorder. References
Angst J., Scharfetter C, Stassen HH: Classification of Schizoaffective Patients by
Multidimensional Scaling and Cluster Analysis. Psychiatria Clin 1983; 16:
254-264
Angst J, Bänninger R, Nüsperli M, Scharfetter C, Stassen HH: Syndromale Gruppierungen endogener
Psychosen in genetischer Sicht. In: Perspektiven der Schizophrenie-Forschung, ed: Pflug B.,
Foerster K., Straube E.; Fischer, Stuttgart New York, 1985: 25-38
Stassen HH, Scharfetter C, Angst J: Morbid risks of subgroups of affective disorders: some
methodological and empirical results. J Psychiat Research 1987; 21: 347-355
Stassen HH, Scharfetter C, Winokur G, Angst J: Familial syndrome patterns in schizophrenia,
schizoaffective disorder, mania and depression. Eur Arch Psychiatr Neurol Sci 1988; 237:
115-123
Angst J, Stassen HH, Gross G, Huber G, Stone MH: Suicide in affective and schizoaffective
disorders. In: Marneros A. and Tsuang M.T. (eds) Affective and Schizoaffective disorders.
Springer, Berlin-Heidelberg 1990: 168-185
Stassen HH, Schmid GB, Gross G, Angst J, Huber G: Prädiktoren des langfristigen Verlaufs
schizophrener Erkrankungen. In: G. Huber (ed), Idiopathische Psychosen: Psychopathologie,
Neurologie, Therapie. Schattauer, Stuttgart-New York, 1990: 95-104
Scharfetter C, Stassen HH: Psychopathological concepts. Psychopathology 1995; 28: 8-12
Stassen HH, Ragaz M, Reich T: Age-of-onset or age-cohort changes in the lifetime occurrence of
depression? Psychiat Genetics 1997; 7: 27-34
Angst J, Stassen HH: Methodische Probleme der Prüfung von Antidepressiva. In: Stieglitz RD,
Fähndrich E, Möller HJ (eds): Syndromale Diagnostik psychischer Störungen. Hogrefe, Göttingen
1998: 5-12
Angst J, Angst F, Stassen HH: Suicide risk in patients with major depressive disorder. J Clin
Psychiatry 1999; 60,2: 57-62
Angst F, Stassen HH, Clayton PJ, Angst J: Mortality of patients with mood disorders: follow-up
over 34 to 38 years. J Aff Disorders 2002; 68: 167-181
Stassen HH: Veränderungen der Sprechmotorik. In: T.Jahn (ed) Bewegungsstörungen bei psychischen
Erkrankungen. Springer Heidelberg 2004: 107-125
Angst J, Sellaro R, Stassen HH, Gamma A: Diagnostic conversion from depression to bipolar
disorders: results of a long-term prospective study of hospital admissions. J Aff Disorders
2005; 84(2-3): 149-157
Stassen HH, Angst J, Scharfetter C, Szegedi A: Therapie mit Antidepressiva: Erfolg von
genetischen Faktoren abhängig? Leading Opinions, Neurologie & Psychiatrie 2005; 6: 25-27
Stassen HH, Scharfetter C: Ethnische Zugehörigkeit und Vulnerabilität am Beispiel der
Affektkrankheiten und Schizophrenien. Die Psychiatrie 2005; 2: 85-95
Stassen HH, Angst J, Scharfetter C: Genetik affektiver Störungen —der quantitative Ansatz
syndrom-orientierter Modelle. In: M. Leuzinger-Bohleber, S. Hau, H. Deserno (hsg): Depression
—Pluralismus in Praxis und Forschung, Vandenhoeck & Ruprecht, Göttingen, 2005, pp. 219-257
Stassen HH, Scharfetter C, Angst J: Functional Psychoses —Molecular-genetic Evidence for a
Continuum. In: A. Marneros and H.S. Akiskal (eds) The overlap of affective and schizophrenic
spectra. Cambridge University Press 2006; pp. 55-78
Stassen HH, Scharfetter C: Vulnerability, resilience and response to psychotropic drugs:
shared genetic factors? Am J Med Genetics 2006; 141: 707-708
Stassen HH, Angst J, Hell D, Scharfetter C, Szegedi A: Is there a common resilience mechanism
underlying antidepressant drug response? Evidence from 2848 patients. J Clin Psychiatry
2007; 68(8): 1195-1205
|
|
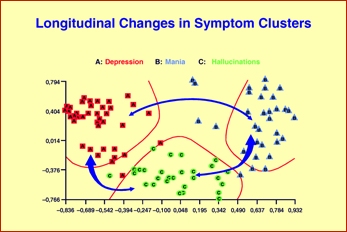
Marked fluctuations in the symptom/syndrome patterns of psychiatric patients can be observed over multiple episodes. Though relevant to the time course of the illness and the patients' long-term prognosis, such fluctuations are insufficiently covered by the schemata of clinical diagnoses.
Please note: no more than 10% of patients show stable symptom/syndrome patterns
over multiple episodes.
|
|
| [ Mail to Webmaster ] k454910@ifrg.ch |
|