Professor Dr. med. Christian ScharfetterDept. of Psychiatry, Psychotherapy & PsychosomaticsPsychiatric Hospital, University of Zurich |
|
|
Efficacy of AntidepressantsCurrent knowledge about the mechanisms of action of antidepressants is rather limited. In consequence, it is not possible to make any predictions of whether or not a particular patient will respond to a particular treatment. The most puzzling point in the treatment of Major Depressive Disorder (MDD), however, is the observation that antidepressants which differ greatly in their biochemical design and primary site of pharmacological action display virtually the same efficacy, as measured by the proportion of patients in whom they induce a therapeutic response. Moreover, responder rates are modest, as revealed by recent meta-analyses of FDA data on 10,030 patients from 52 antidepressant drug trials, where active substances showed superiority to placebo in fewer than half of the studies [Khan et al. 2001, 2002]. And, what is particularly difficult to understand: while newer treatments have better tolerability and safety profiles, they do not offer any advantage in either efficacy or their ability to reduce residual symptoms. Mechanisms of ActionWhat might explain the relative lack of progress in the field of antidepressant drug research over the past decades? Antidepressants are hypothesized to achieve their effect through modifications of single (or multiple) targets within the monoaminergic systems. However, a significant amount of clinical data suggest that effective antidepressants act in a rather unspecific and indirect way, that is, to merely trigger and maintain conditions necessary for recovery in a subgroup of patients who otherwise would remain nonresponders. Once triggered, the recovery of these patients follows its "natural" course as equally observed under placebo treatment. Indeed, antidepressants appear to be "polyvalent" in the sense that they induce a therapeutic response under various clinical indications. For example, antidepressants are also effective in anxiety disorders and antipsychotics are successfully used in the treatment of bipolar illness. Advanced ApproachesIt is quite unlikely that the observed inter-individual variation of antidepressant drug response "results" from one single factor or a few major factors, as single gene approaches typically "explain" no more than a small percentage <1.5% of observed variance. In consequence, advanced molecular-genetic approaches to psychotropic drug response involve (1) configurations of a larger number of interacting factors, and (2) quantitative phenotypes that assess more than just the rudimentary response-nonresponse dichotomy. References
Angst J, Stassen HH, Woggon B: Effect of neuroleptics on positive and negative symptoms and
the deficit state. Psychopharmacology 1989; 99: 41-46
Angst J, Delini-Stula A, Stabl M, Stassen HH: Is a cutoff score a suitable measure of
treatment outcome in short-term trials in depression? A methodological meta-analysis.
Human Psychopharmacology 1993; 8: 311-317
Stassen HH, Delini-Stula A, Angst J: Time course of improvement under antidepressant treatment:
a survival-analytical approach. Eur Neuropsychopharmacol 1993; 3: 127-135
Stassen HH, Angst J, Delini-Stula A: Severity at baseline and onset of improvement in depression.
Meta-analysis of Imipramine and Moclobemide vs Placebo. Eur Psychiatry 1994; 9: 129-136
Stassen HH, Angst J: Methods of estimating onset of improvement. Eur Neuropsychopharmacology
1994; 4,3: 284-285
Kuny S, Stassen HH: Cognitive performance in patients recovering from depression. Psychopathology
1995; 28: 190-207
Stassen HH, Angst J, Delini-Stula A: Delayed onset of action of antidepressant drugs? Survey of
results of Zurich meta-analyses. Pharmacopsychiatry 1996; 29: 87-96
Stassen HH, Angst J, Delini-Stula A: Delayed onset of action of antidepressant drugs? Survey
of results of Zurich meta-analyses. Eur Psychiatry 1997; 12: 166-176
Angst J, Stassen HH: Methodische Probleme der Prüfung von Antidepressiva. In: Stieglitz RD,
Fähndrich E, Möller HJ (eds): Syndromale Diagnostik psychischer Störungen. Hogrefe, Göttingen
1998: 5-12
Stassen HH, Angst J, Delini-Stula A: Onset of improvement under fluoxetine and moclobemide.
Eur Psychiatry 1998; 13,3: 128-133
Stassen HH, Kuny S,. Hell D: The speech analysis approach to determining onset of improvement
under antidepressants. Eur Neuropsychopharmacology 1998; 8,4: 303-310
Stassen HH, Angst J, Delini-Stula A: Fluoxetine versus moclobemide: cross-comparison between the
time course of improvement. Pharmacopsychiatry 1999; 32: 56-60
Montgomery SA, Bech P, Blier P, Moller HJ, Nierenberg AA, Pinder RM, Quitkin FM, Reimitz PE,
Rosenbaum JF, Rush AJ, Stassen HH, Thase ME: Selecting methodologies for the evaluation of
differences in time to response between antidepressants. J Clin Psychiatry 2002; 63(8):
694-699
Stassen HH, Dahmen N, Hell D, Nürnberg P, Sander T, Toliat MR, Szegedi A: Genetic predisposition
of antidepressant drug response. Am J Med Genetics 2003; 122: 123-124
Stassen HH, Angst J: Wirkung und Wirkungseintritt in der Antidepressiva-Behandlung.
Medizinspektrum 2004; 15: 15-17
Stassen HH, Angst J, Scharfetter C, Szegedi A: Therapie mit Antidepressiva: Erfolg von
genetischen Faktoren abhängig? Leading Opinions, Neurologie & Psychiatrie 2005; 6: 25-27
Lavergne F, Berlin I, Gamma A, Stassen H, Angst J: Onset of improvement and response to
mirtazapine in depression: a multicenter naturalistic study of 4771 patients. Neuropsychiatric
Disease and Treatment 2005; 1(1): 59-68
Stassen HH, Scharfetter C: Vulnerability, resilience and response to psychotropic drugs:
shared genetic factors? Am J Med Genetics 2006; 141: 707-708
Stassen HH, Angst J, Hell D, Scharfetter C, Szegedi A: Is there a common resilience mechanism
underlying antidepressant drug response? Evidence from 2848 patients. J Clin Psychiatry 2007;
68(8): 1195-1205
Szegedi A, Jansen WT, Van Willigenburg AP, Van der Meulen E, Stassen HH, Thase ME: Early
improvement as a predictor of treatment outcome in patients with major depressive disorder:
Why the first 2 weeks really matter - evidence from 6562 patients. J Clin Psychiatry 2009; 70(3): 344-353
Lötscher K, Anghelescu IG, Braun S, Bridler R, Stassen HH: Polypharmacy in psychiatry: clinical practice
versus empirical evidence. Eur Neuropsychopharmacol. 2010; 20 (Suppl. 3): 378-379
Kemp DE, Ganocy SJ, Brecher M, Carlson BX, Edwards S, Eudicone JM, Evoniuk G, Jansen W, Leon AC,
Minkwitz M, Pikalov A, Stassen HH, Szegedi A, Tohen M, Van Willigenburg AP, Calabrese JR: Clinical value
of early partial symptomatic improvement in the prediction of response and remission during short-term
treatment trials in 3369 subjects with bipolar I or II depression. J Affect Disord. 2011; 130(1-2): 171-179
Stassen HH, Anghelescu IG, Angst J, Böker H, Lötscher K, Rujescu D, Szegedi A, Scharfetter C:
Predicting Response to Psychopharmacological Treatment. Survey of Recent Results.
Pharmacopsychiatry 2011; 44: 263-272
|
|
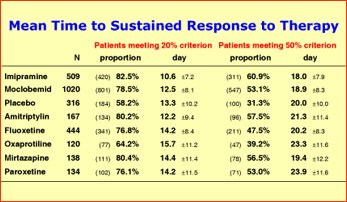
Time points of sustained improvement and sustained response in the "average" patient under antidepressant and placebo treatment, as derived from an "individual-case" analysis using "true" assessment days rather than the "design days" of the study protocols. Differences between treatment modalities appear to relate to the proportion of patients in whom a therapeutic effect is induced but not to the onset of effect.
Please note: (1) mean time to onset of improvement is approximately 12 days for all
treatment modalities (sustained 20% baseline score reduction); (2) time to response is approximately
20 days for all treatment modalities (sustained 50% baseline score reduction).
|
|
| [ Mail to Webmaster ] k454910@ifrg.ch |
|