Professor Dr. med. Christian ScharfetterDept. of Psychiatry, Psychotherapy & PsychosomaticsPsychiatric Hospital, University of Zurich |
|
|
The Burden of Acute and Long-Term Side EffectsIn tandem with the benefits of antipsychotic medications are significant risks associated with their use. These risks are primarily acute and chronic neurological adverse effects, such as parkinsonism, akathisia, dystonia, and tardive dyskinesia, that can range in intensity from mild to severe. Newer atypical antipsychotic agents do not cause agranulocytosis, and usually cause fewer parkinsonian symptoms than the typical agents when given in doses at the lower end of their therapeutic range. Side effects include (1) acute dystonic reaction (2% of patients, onset within hours); (2) drug-induced Parkinsonism (20-40% of patients, onset 5-30 days); (3) akathisia (20% of patients, onset 5-60 days); (4) tardive dyskinesia (20% of patients, onset 3 months to years); (5) neuroleptic malignant syndrome (0.5-1% of patients, mortality around 20%); (6) metabolic impairments among which weight gain (15% of patients within the first weeks of treatment — 50% of patients in the long term) and diabetis mellitus (6% of patients) are prominent. Highly Compromised ComplianceAcute side effects of antipsychotics, generally referred to as extrapyramidal side effects, are often quite uncomfortable for patients and may compromise compliance with an otherwise beneficial antipsychotic medication regimen. Extrapyramidal effects by themselves have been related to a poor outcome, a compromised compliance, secondary negative symptoms, cognitive parkinsonism, and depression. PharmacogeneticsAntipsychotic-induced extrapyramidal effects, along with the conditions under which they occur in the individual patient, are insufficiently understood, and display considerable ethnic variation. Given current knowledge, it is not possible to make any predictions of whether a particular patient will develop side effects — and to what extent — under a particular antipsychotic treatment. Clearly, the assessment of ethnicity-specific predictors by means of objective laboratory methods would greatly improve antipsychotic drug therapies and ultimately lead to a more personalized and better tolerable medicine. References
Agid O, Kapur S, Arenovich T, Zipursky RB. Delayed-onset hypothesis of antipsychotic
action: a hypothesis tested and rejected. Arch Gen Psychiatry 2003; 60(12): 1228-1235
Agid O, Seeman P, Kapur S. The "delayed onset" of antipsychotic action--an idea whose
time has come and gone. J Psychiatry Neurosci. 2006; 31(2): 93-100
Agid O, Kapur S, Warrington L, Loebel A, Siu C. Early onset of antipsychotic response
in the treatment of acutely agitated patients with psychotic disorders. Schizophr Res.
2008; 102(1-3): 241-248
Cassano P, Fava M. Tolerability issues during long-term treatment with antidepressants.
Ann Clin Psychiatry 2004; 16(1): 15-25
Chwastiak LA, Rosenheck RA, McEvoy JP, Keefe RS, Swartz MS, Lieberman JA.
Interrelationships of psychiatric symptom severity, medical comorbidity, and
functioning in schizophrenia. Psychiatr Serv. 2006; 57(8): 1102-1109
Correll CU, Malhotra AK. Pharmacogenetics of antipsychotic-induced weight gain.
Psychopharmacology 2004; 174(4): 477-489
Eaton WW, Byrne M, Ewald H, Mors O, Chen CY, Agerbo E, Mortensen PB. Association of
schizophrenia and autoimmune diseases: linkage of Danish national registers. Am J
Psychiatry 2006; 163(3): 521-528
Fleischhacker WW, Cetkovich-Bakmas M, De Hert M, Hennekens CH, Lambert M, Leucht S,
Maj M, McIntyre RS, Naber D, Newcomer JW, Olfson M, Osby U, Sartorius N, Lieberman JA.
Comorbid somatic illnesses in patients with severe mental disorders: clinical, policy,
and research challenges. J Clin Psychiatry. 2008;69(4): 514-519
Geddes J, Freemantle N, Harrison P, Bebbington P. Atypical antipsychotics in the treatment of
schizophrenia: systematic overview and meta-regression analysis. BMJ 2000; 321(7273): 1371-1376
Häfner H. Ist die Diagnose Schizophrenie noch sinnvoll? Psychiat Prax 2007; 34: 175-180
Khan A, Khan SR, Leventhal RM, Brown WA. Symptom reduction and suicide risk in patients
treated with placebo in antidepressant clinical trials: a replication analysis of the
Food and Drug Administration Database. Int J Neuropsychopharmacol 2001; 4(2): 113-118
Khan A, Khan SR, Leventhal RM, Brown WA. Symptom reduction and suicide risk among
patients treated with placebo in antipsychotic clinical trials: an analysis of the
food and drug administration database. Am J Psychiatry 2001; 158(9): 1449-1454
Lett HS, Blumenthal JA, Babyak MA, Sherwood A, Strauman T, Robins C et al. Depression
as a risk factor for coronary artery disease: evidence, mechanisms, and treatment.
Psychosom Med 2004; 66(3): 305-315
Leucht S, Pitschel-Walz G, Abraham D, Kissling W. Efficacy and extrapyramidal side-effects of
the new antipsychotics olanzapine, quetiapine, risperidone, and sertindole compared to
conventional antipsychotics and placebo. A meta-analysis of randomized controlled trials.
Schizophr Res 1999; 35(1): 51-68
Leucht S, Busch R, Kissling W, Kane JM. Early prediction of antipsychotic nonresponse
among patients with schizophrenia. J Clin Psychiatry. 2007; 68(3): 352-360
Li M, Fletcher PJ, Kapur S. Time course of the antipsychotic effect and the
underlying behavioral mechanisms. Neuropsychopharmacology. 2007; 32(2): 263-272
Motivala SJ, Sarfatti A, Olmos L, Irwin MR. Inflammatory markers and sleep disturbance
in major depression. Psychosom Med. 2005; 67(2): 187-194
Papakostas GI, Perlis RH, Scalia MJ, Petersen TJ, Fava M. A meta-analysis of early
sustained response rates between antidepressants and placebo for the treatment of
major depressive disorder. J Clin Psychopharmacol 2006; 26(1): 56-60
Posternak MA, Zimmerman M. Is there a delay in the antidepressant effect? A
meta-analysis. J Clin Psychiatry 2005; 66(2): 148-158
Rudisch B, Nemeroff CB. Epidemiology of comorbid coronary artery disease and
depression. Biol Psychiatry 2003; 54: 227-240
Skilton MR, Moulin P, Terra JL, Bonnet F. Associations between anxiety, depression,
and the metabolic syndrome. Biol Psychiatry. 2007; 62(11): 1251-1257
Stassen HH, Angst J, Hell D, Scharfetter C, Szegedi A. Is there a common resilience
mechanism underlying antidepressant drug response? Evidence from 2848 patients. J
Clin Psychiatry. 2007; 68(8): 1195-1205
Szegedi A, Jansen WT, Van Willigenburg AP, Van der Meulen E, Stassen HH, Thase ME: Early
improvement as a predictor of treatment outcome in patients with major depressive disorder:
Why the first 2 weeks really matter —evidence from 6562 patients. J Clin Psychiatry 2008 (in press)
|
|
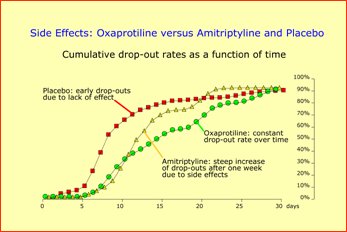
Cumulative rates of premature withdrawals under amitriptyline (TCA; yellow triangles) and oxaprotiline (investigational noradrenaline uptake inhibitor; green circles) versus placebo (red squares). Premature withdrawals occur early under placebo (lack of effect), while drop-outs under amitriptyline typically occur after one week of treatment when dosages reach therapeutical levels. This in contrast to the reduced, unspecific side effect profile of oxaprotiline, where premature withdrawals occur at a constant rate over the entire observation period. |
|
| [ Mail to Webmaster ] k454910@ifrg.ch |
|