Professor Dr. med. Christian ScharfetterDept. of Psychiatry, Psychotherapy & PsychosomaticsPsychiatric Hospital, University of Zurich |
|
|
Shared Genetic FactorsThe utility of current diagnostic entities for genetic studies seems limited, since psychiatric diagnoses incompletely cover the patients' prodromal phase, age-of-onset, severity of illness, long-term course, and impairment. In particular, psychiatric diagnoses do not offer much information about a patient's response to treatment and prognosis. Evidence from quite a number of studies suggests significant interrelationships between vulnerability to major psychiatric disorders, resilience factors, medical comorbidity, and the time course of recovery under antidepressants and antipsychotics. Shared genetic factors appear to increase or decrease the likelihood for developing the disorders, as they appear to support or impede recovery. Quantitative, syndrome-oriented approaches to psychopathology replace the dichotomy of the diagnostic schema by dimensional quantities and allow one to evaluate "psychopathological similarity" between patients across diagnostic boundaries. Support from Molecular-Genetic StudiesSeveral previous investigations have suggested that the gene for the α7-nicotinic receptor may play a role in the pathogenesis of schizophrenia and may be responsible for heavy smoking among schizophrenic patients. In a study of 129 healthy controls and 127 schizophrenic, schizoaffective and bipolar patients, we aimed (1) to confirm the potential association between schizophrenia and the α7-nicotinic receptor, (2) to test the diagnostic specificity of α7-receptor subunits with respect to psychiatric diagnoses, and (3) to investigate potential receptor differences between smokers and nonsmokers in the general population. Our analysis included the two dinucleotide polymorphisms D15S1360 and L76630 that are localized in a genomic fragment containing the α7-nicotinic receptor gene CHRNA7. Highly significant differences (p < 0.0001) between the allele distributions of patients and controls were detected for these two markers, with all three diagnostic subgroups contributing to the discrimination. An independently ascertained replication sample of 24 patients confirmed this finding (Table). Unresolved Methodological IssuesThe genetic analysis of complex disorders influenced by multiple genes as well as multiple non-genetic factors is a still unresolved methodological issue. Standard phenotype-to-genotype research strategies enable the localization of genes coding for traits influenced by a few major genes. Yet these strategies have not been successful in elucidating the genetic background of complex disorders. Thus, if (1) the contributions of single loci are small, (2) the single loci are, by themselves, neither necessary nor sufficient for developing the phenotype, (3) significant interactions between the loci are involved, and (4) there exist different pathways to the phenotype in ethnically different populations, detecting genes by these strategies may be very difficult or impossible. Unknown population admixture can also substantially reduce the power of studies that aim to link phenotype to genotype. References
Angst J., Scharfetter C, Stassen HH: Classification of Schizoaffective Patients by
Multidimensional Scaling and Cluster Analysis. Psychiatria Clin 1983; 16:
254-264
Angst J, Bänninger R, Nüsperli M, Scharfetter C, Stassen HH: Syndromale Gruppierungen endogener
Psychosen in genetischer Sicht. In: Perspektiven der Schizophrenie-Forschung, ed: Pflug B.,
Foerster K., Straube E.; Fischer, Stuttgart New York, 1985: 25-38
Stassen HH, Scharfetter C, Angst J: Morbid risks of subgroups of affective disorders: some
methodological and empirical results. J Psychiat Research 1987; 21: 347-355
Stassen HH, Scharfetter C, Winokur G, Angst J: Familial syndrome patterns in schizophrenia,
schizoaffective disorder, mania and depression. Eur Arch Psychiatr Neurol Sci 1988; 237:
115-123
Angst J, Stassen HH, Gross G, Huber G, Stone MH: Suicide in affective and schizoaffective
disorders. In: Marneros A. and Tsuang M.T. (eds) Affective and Schizoaffective disorders.
Springer, Berlin-Heidelberg 1990: 168-185
Stassen HH, Schmid GB, Gross G, Angst J, Huber G: Prädiktoren des langfristigen Verlaufs
schizophrener Erkrankungen. In: G. Huber (ed), Idiopathische Psychosen: Psychopathologie,
Neurologie, Therapie. Schattauer, Stuttgart-New York, 1990: 95-104
Scharfetter C, Stassen HH: Psychopathological concepts. Psychopathology 1995; 28: 8-12
Stassen HH, Ragaz M, Reich T: Age-of-onset or age-cohort changes in the lifetime occurrence of
depression? Psychiat Genetics 1997; 7: 27-34
Angst J, Stassen HH: Methodische Probleme der Prüfung von Antidepressiva. In: Stieglitz RD,
Fähndrich E, Möller HJ (eds): Syndromale Diagnostik psychischer Störungen. Hogrefe, Göttingen
1998: 5-12
Angst J, Angst F, Stassen HH: Suicide risk in patients with major depressive disorder. J Clin
Psychiatry 1999; 60,2: 57-62
Angst F, Stassen HH, Clayton PJ, Angst J: Mortality of patients with mood disorders: follow-up
over 34 to 38 years. J Aff Disorders 2002; 68: 167-181
Stassen HH: Veränderungen der Sprechmotorik. In: T.Jahn (ed) Bewegungsstörungen bei psychischen
Erkrankungen. Springer Heidelberg 2004: 107-125
Angst J, Sellaro R, Stassen HH, Gamma A: Diagnostic conversion from depression to bipolar
disorders: results of a long-term prospective study of hospital admissions. J Aff Disorders
2005; 84(2-3): 149-157
Stassen HH, Angst J, Scharfetter C, Szegedi A: Therapie mit Antidepressiva: Erfolg von
genetischen Faktoren abhängig? Leading Opinions, Neurologie & Psychiatrie 2005; 6: 25-27
Stassen HH, Scharfetter C: Ethnische Zugehörigkeit und Vulnerabilität am Beispiel der
Affektkrankheiten und Schizophrenien. Die Psychiatrie 2005; 2: 85-95
Stassen HH, Angst J, Scharfetter C: Genetik affektiver Störungen —der quantitative Ansatz
syndrom-orientierter Modelle. In: M. Leuzinger-Bohleber, S. Hau, H. Deserno (hsg): Depression
—Pluralismus in Praxis und Forschung, Vandenhoeck & Ruprecht, Göttingen, 2005, pp. 219-257
Stassen HH, Scharfetter C, Angst J: Functional Psychoses —Molecular-genetic Evidence for a
Continuum. In: A. Marneros and H.S. Akiskal (eds) The overlap of affective and schizophrenic
spectra. Cambridge University Press 2006; pp. 55-78
Stassen HH, Scharfetter C: Vulnerability, resilience and response to psychotropic drugs:
shared genetic factors? Am J Med Genetics 2006; 141: 707-708
Stassen HH, Angst J, Hell D, Scharfetter C, Szegedi A: Is there a common resilience mechanism
underlying antidepressant drug response? Evidence from 2848 patients. J Clin Psychiatry
2007; 68(8): 1195-1205
|
|
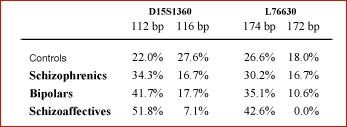
Results suggested a nonspecific, α7-related vulnerability to functional psychoses which depended on the severity of overall psychopathology, with no clear-cut boundary between clinical diagnoses. This vulnerability was lowest among schizophrenics, intermediate among bipolars, and highest among schizoaffectives. For the healthy control subjects, we found no association between the α7-nicotinic receptor gene and tobacco consumption and, consequently, no evidence that the differences between patients and controls could be explained through a genetic predisposition to tobacco consumption.
Please note: (1) the α7-nicotinic receptor gene explains less than 1.5% of the
observed phenotypic variance; (2) single gene effects are generally small for complex disorders in the
range of 0.5-1.5% explained variance; (3) single gene effects are non-additive; (4) interactions
between genomic loci exceed main effects by far (up to 7-fold); (5) significances originate
from small subgroups of patients and are difficult to reproduce.
|
|
| [ Mail to Webmaster ] k454910@ifrg.ch |
|