EUTwinsS: Twins with SchizophreniaInstitute for Response-Genetics, University of ZurichHead: Prof. Dr. Hans H. Stassen |
|
Partners:
|
Normative Study of Healthy Twin PairsWe have carried out a sufficiently representative study of healthy twins in order to systematically investigate the issue of within-pair concordance in monozygotic (mz) and dizygotic (dz) twins [Lykken and Stassen: data of 1,300 dz and 1,434 mz twin pairs]. By definition, the genetic similarity between mz co-twins is "1" and that of dz co-twins "0.5". On the phenotype level, however, the concordance of mz and dz co-twins follows a normal distribution with mean values and variances ("norm of reaction"). In particular, the dz concordance can vary from complete dissimilarity (comparable unrelated individuals) and perfect similarity (comparable to mz co-twins). The analysis of quantitative traits "finger ridge count", "body height", "brain-wave patterns", "shoe size", and "body weight" yield almost perfect mz:dz ratios of 2:1, thus suggesting an additive genetic model in the background (Table). In that case the mz concordance gives the size of the genetic backgound (e.g., 82% of the observed inter-individual variance of barinwave patterns is explainable by genetic factors). Significant deviations from the 2:1 ratio indicate a more complex interplay between environment and genetic factors. For example, several IQ dimensions display the same high concordances for dz and mz co-twins, thus suggesting dominant environmental factors. 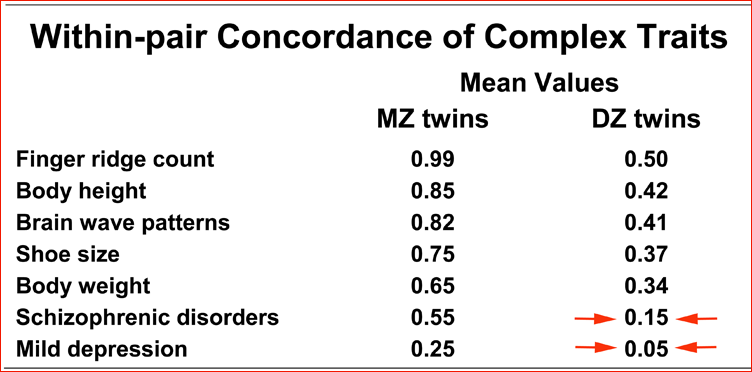
Quantitative Syndrome-Oriented Approaches to PsychopathologyMajor psychiatric disorders are familial in the sense that they "run" in families but they do not seggregate. In fact, the underlying vulnerability acts unspecificly and is neither a necessary nor a sufficient condition for developing a psychiatric disorder or a particular clinical diagnosis. The phenotypical picture is not homotypic in terms of clinical diagnoses, for example, we frequently observe first degree relatives with a diagnosis of depression in families ascetrained through index cases with a diagnosis of schizophrenia. Quantitative syndrome-oriented approaches apparently offer advantages over the qualitative taxonomy of diagnostic systems. Specifically, multidimensional syndrome patterns have turned out (1) to resolve the fine gradations of within-family psychopathologies that do not reach diagnostic thresholds, and (2) to relate to the time course of recovery under psychotropic drug treatment. Twins with SchizophreniaQuantitative sychopathology syndrome scores suggest that mz co-twins who shared the same environment have a 3.7-fold higher risk to both suffer from schizophrenic disorders, compared to dz co-twins raised together (Table). Significant deviations from the mz:dz ratio of 2:1 indicate the existence of strong non-linearities which are typical for self-regulating systems, such as the monoaminergic systems or the inflammatory response system. In fact, there is evidence that mz co-twins concordant for schizophrenia may possess a less "robust" variant of the inflammatory response system that can more easily be triggered by exogenous factors compared to the more "robust" variants postulated for mz co-twins discordant for schizophrenia. Moreover, data from 753 patients under antidepressants or antipsychotics suggest that up to 15% of the response to antidepressants and up to 25% of the response to antipsychotics might be explainable through the inflammatory response system. |
|
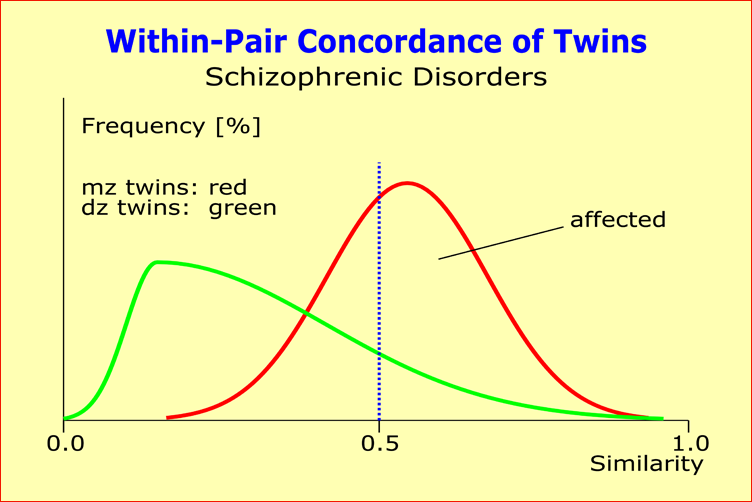
Within-pair concordances of psychopathology syndrome scores in mz and dz twins where at least one co-twin suffers from schizophrenic disorder. No more than 55% of mz and 15% of dz co-twins are concordant for schizophrenia, thus displaying significant deviations from the mz:dz ratio of 2:1.
Detailed analyses of our family data showed that: (1) patients with a clinical diagnosis of
schizoaffective disorders have the highest genetic vulnerability; (2) the genetic vulnerability
depends on the age of onset and the severity of psychopathology scores;
(3) genetic vulnerability appears to be ethnicity-independent.
|
|
| [ Mail to Webmaster ] k454910@ifrg.ch |
|